How many lives can a low-cost, low-tech package of intrapartum and immediate newborn care interventions save?
Even in low-resource settings, with no grand changes in existing manpower, resources, or technology, a carefully designed package of interventions increased the 28-day survival of preterm or low-birth-weight babies by 34%.
Preterm birth, or birth before 37 weeks of gestation, is the leading cause of death in children under five years old and is the strongest risk factor for early neonatal death. In Kenya and Uganda, specifically, while annual neonatal mortality rates have ticked down over the last decade, they remain high at 20-26 per 1,000 live births 1
. Those who survive preterm birth are at risk for long-term disability and chronic health issues, often leaving families and communities wrestling with ongoing health, social and financial burdens. While many perinatal evidence-based interventions exist, and may even be formally adopted into policy guidelines, it is still estimated that up to two-thirds of neonatal deaths in high-burden countries could be averted with improved care during and immediately after birth 2
. In order for existing interventions to achieve their desired impact of preventing neonatal mortality, these estimates suggest that interventions, when implemented together rather than individually, can significantly improve outcomes. However, many proven interventions are not widely used in many low- and middle-income settings because of financial resource and workforce capacity limitations and cultural or social barriers. Low-cost interventions, while often perceived as basic, can be more practical solutions to real-world problems. Thus, Preterm Birth Initiative East Africa (PTBi EA) invested in reinforcing what a health system already has and focused on quality of care and promotion of evidence-based practices that are known, but not routinely used. This research also investigated the impact of implementing multiple interventions together, rather than individually or in a pair.
Design
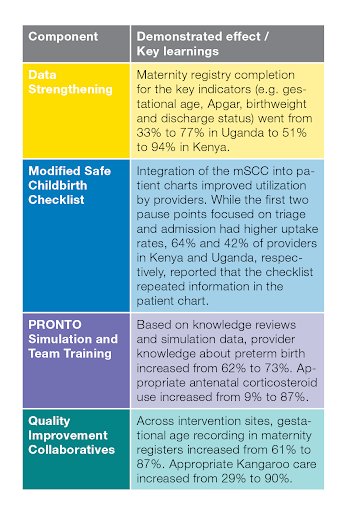
With the assistance of Kenya and Uganda’s Ministries of Health and local health authorities and volunteers in Migori County and the Busoga Region, the PTBi EA team developed and tested an intervention package that contained four core components: data strengthening, a modified WHO Safe Childbirth Checklist, PRONTO simulation and team training, and Quality Improvement (QI) Collaboratives. The data strengthening intervention included reinforcing key indicator definitions, reviewing gestational age assignment, and providing a platform for ongoing data feedback and mentoring. For the mSCC intervention, researchers modified the WHO Safe Childbirth Checklist to align with each country’s national guidelines, adapted the implementation strategies to local settings, and added reminders about preterm labor identification and preterm infant care. The PRONTO intervention was an emergency obstetric and neonatal care simulation-based training that emphasized the identification, triage, and management of preterm labor and birth while aiming to increase uptake of evidence-based practices and strengthen communication and teamwork among facility teams. The QI Collaboratives were periodic meetings of facility-based QI teams that implemented Plan-Do-Study-Act cycles to overcome system bottlenecks and to track core QI indicators related to preterm birth. To evaluate the effect of the full intervention package on preterm mortality, researchers conducted a cluster-randomized controlled trial among 20 public sector health facilities in the Busoga Region of Uganda and Migori County, Kenya. Ten control facilities received data strengthening and the mSCC, whereas ten intervention facilities received all four components of the package. The study group included infants born alive weighing between 1,000g and 2,500g, or less than 3,000g with a recorded gestational age less than 37 weeks, and fresh stillbirths meeting the same eligibility criteria.
Impact
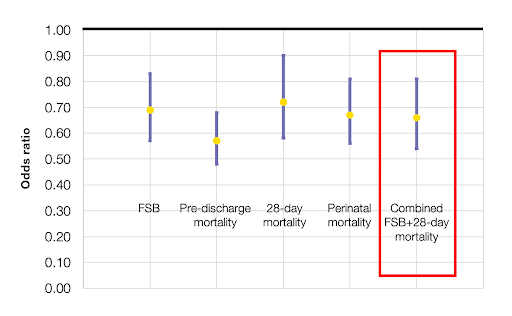
Study-eligible babies born in hospitals receiving the full intervention package had 34% greater odds of surviving to 28 days, compared to eligible babies born in hospitals that did not receive the intervention package For the primary outcome, 23.3% (347/1,491) of control group eligible infants were stillborn or died in the neonatal period compared with 15.3% (221/1,447) in the intervention group, as seen in the figure below.
Figure 1: Reduced mortality odds amongst eligible births was significant across all outcomes
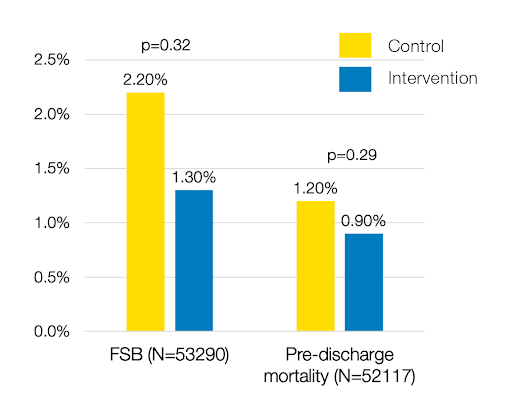
All births may have benefited from exposure to the intervention package
The intervention package similarly showed a trend toward reductions in fresh stillbirths and pre-discharge mortality among all babies born in intervention hospitals, not just those born preterm or low birthweight.
Figure 2: All births benefitted from the intervention package
The full intervention package also had a positive impact on providers’ confidence and attitudes
In addition to improved preterm outcomes, this intervention also strengthened the capacity and confidence of providers who dealt with preterm labor and newborns--creating a positive reinforcing cycle for long-lasting, sustainable change.
Implementation Guidelines
When developing and implementing their intervention package, the researchers concentrated on factors that relied on existing infrastructure and required minimal new investment, which made the implementation of the package low-cost. For successful implementation, the following three factors were necessary to help create the right environment to transform the culture of care:
Visibility: Counting and valuing women and their preterm babies made this epidemic visible to families, communities, Ministries of Health, researchers, and funders.
Teamwork: Taking appropriate actions and making the right decisions at critical moments requires the accountability that comes with being part of a team, part of a community. Interventions that reinforced teamwork and community principles were vital to this intervention’s success.
Engagement: Including both national stakeholders and local leaders in the intervention’s planning, implementation, and evaluation was vital in ensuring the intervention was accepted and continued after the trial ended.
Lessons Learned
The combination of the intervention package’s different components created a positive reinforcing cycle that added to this intervention's success, sustainability, and uptake.
The intervention package was successful for many, inter-connected reasons that took place during the planning, implementation, and uptake of these interventions. Launching this initiative gave the condition a name, while counting these babies through data strengthening quantified the condition. Strengthening the capacity of the providers to address the condition improved their confidence to act and changed their attitudes towards these small and vulnerable babies. Finally, seeing the improved outcomes through quality improvement activities reinforced that providers were doing the right things.
Through this study, researchers demonstrated that complex problems like preterm birth are better addressed through complex approaches, such as using multiple reinforcing interventions.
Specifically, the inclusion of a simulation and team training and Quality Improvement collaboratives made a significant difference in the intervention package’s success at reducing the burden of preterm birth.
Implications for Future Work
Even in low-resource settings, without significant changes in existing manpower, resources, or technology, this low-cost, low-tech intervention package dramatically improved health outcomes, increased provider capacity, and confidence during intrapartum care, and reduced the burden of prematurity. Using a package of evidence-based interventions that improve the visibility of the problem, build teamwork between providers, and engage national and local stakeholders, you can make a difference in preterm morbidity and mortality.
“It [PRONTO training and mentorship] makes you the have courage when you are handling emergencies, and it is because whenever we have a training you have to go through simulations, it makes you not fear...” – Health worker
“We needed to keep this collaboration alive even after the project… [the MNCH WhatsApp group participants created] is now synonymous with sharing of experiences, peer to peer support, consultations on medical conditions and course of action for the treatment and dosage, improved referral to a health facility that has a particular service… leadership engagement and continuing mentorship, among others.” -- Makerere University Centre of Excellence for Maternal Newborn and Child Health worker