Financial incentives to promote retention in care and viral suppression in adults with HIV initiating antiretroviral therapy in Tanzania
Using a three-arm, parallel-group, randomized controlled trial at four health facilities in Shinyanga region, Tanzania, we studied the impact of varying-sized financial incentives for clinic attendance on viral suppression among patients starting antiretroviral therapy (ART).
Viral suppression is key to ending the HIV epidemic, yet only 58% of people living with HIV (PLHIV) in sub-Saharan Africa are suppressed. Financial incentives promote utilization of HIV services and may support adherence to the sustained antiretroviral therapy (ART) necessary for viral suppression, but few studies have assessed a biomarker of adherence or evaluated optimal implementation. We sought to determine whether varying-sized financial incentives for clinic attendance impact viral suppression among patients starting ART in the Shinyanga region of Tanzania. Shinyanga is located in the Lake Zone region of Tanzania, a rural part of the country where over 4.5 million people live in poverty (32–35% of the population) 1
. Adult HIV prevalence in Shinyanga is 5.9% (4.7% nationally); among those living with HIV in Shinyanga, approximately 40% are virally suppressed (52% nationally) 2
.
Design
We conducted a three-arm parallel-group randomized controlled trial in the Shinyanga region, Tanzania. At four health facilities, HIV-positive adult (≥18 years) ART initiates (≤30 days) were randomly allocated using a tablet-based application (1:1:1, stratified by site) to receive usual care (control group) or to additionally receive a cash incentive for monthly clinic attendance in one of two amounts: 10000 Tanzanian Shillings (TZS) (≈USD 4.50) or 22500 TZS (≈USD 10.00).
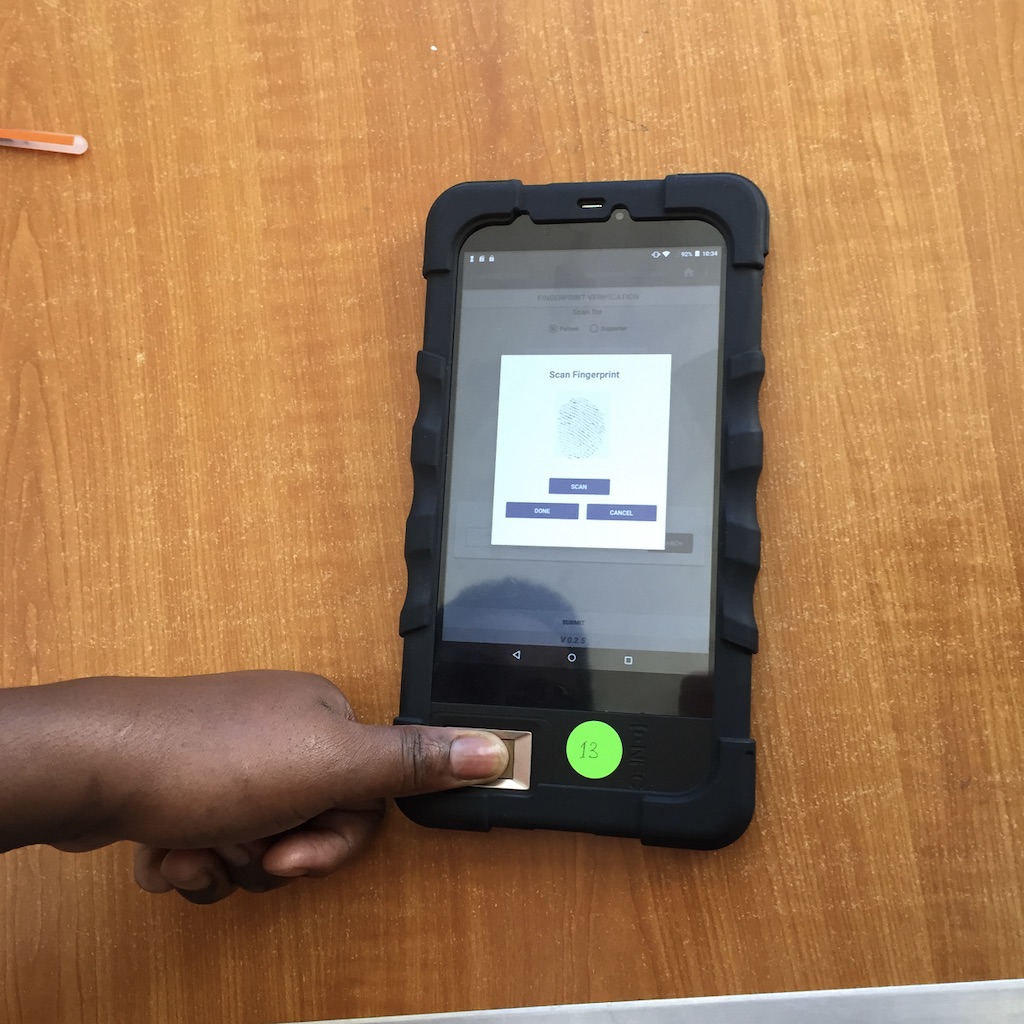
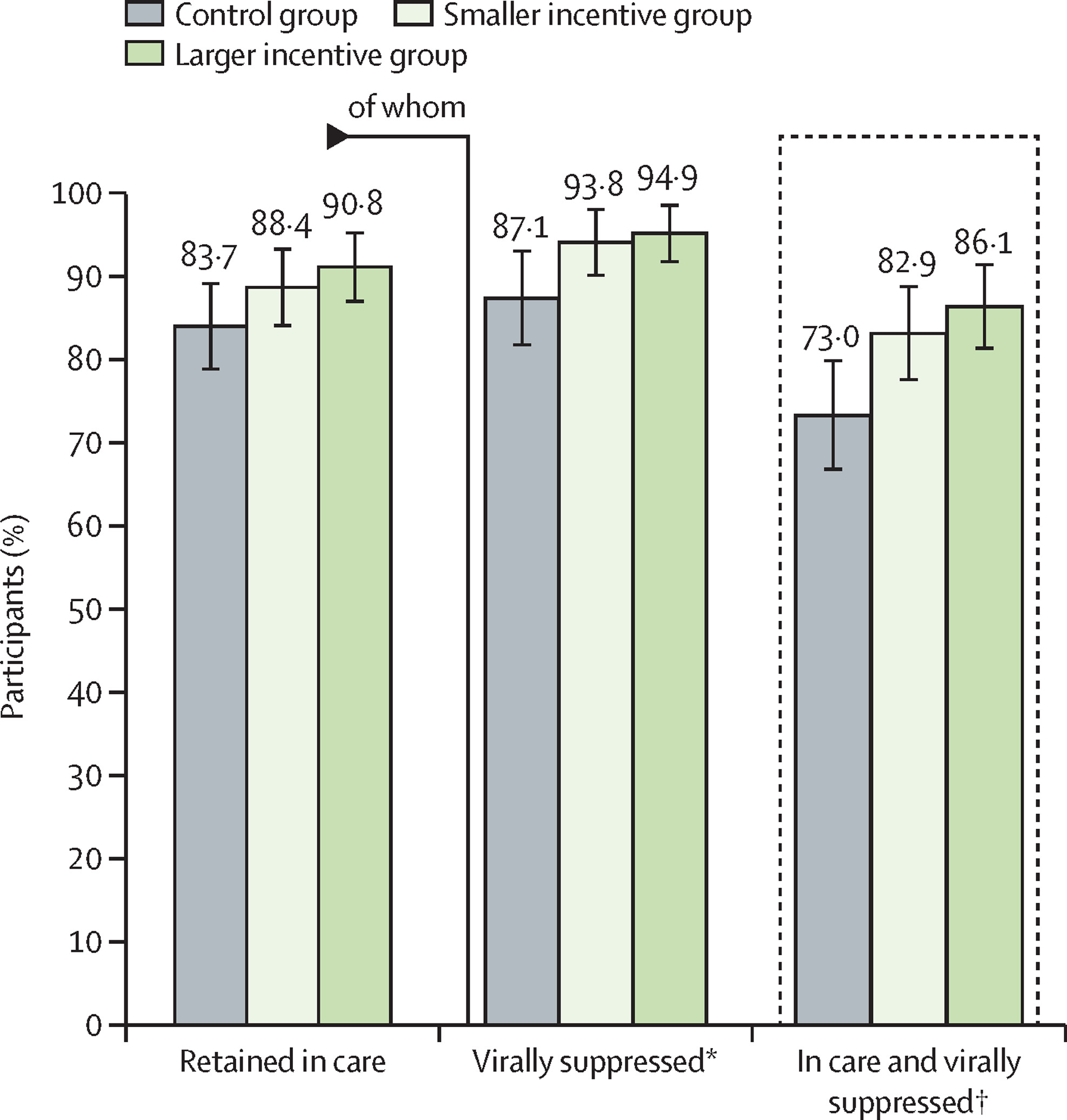
Incentives were provided for up to 6 months via mobile health technology (mHealth) that linked biometric attendance monitoring to automated mobile payments. We evaluated the primary outcome of retention in care with viral suppression (<1000 copies per mL) at 6 months using logistic regression. At 6 months, approximately 134 (73%) participants in the control group remained in care and had viral suppression, compared with 143 (83%) in the smaller incentive group (risk difference [RD] 9·8, 95% CI 1·2 to 18·5) and 150 (86%) in the larger incentive group (RD 13·0, 4·5 to 21·5); we identified a positive trend between incentive size and viral suppression (p trend=0·0032), although the incentive groups did not significantly differ (RD 3·2, −4·6 to 11·0).
In addition to the RCT, we conducted a mixed-methods process evaluation guided by the Proctor implementation science framework.
Impact
At six months, 134 (73%) of PLHIV in the control group remained in care and achieved viral suppression, compared to 143 (82.9%) in the smaller incentive group and 150 (86.1%) in the larger incentive group; we identified a positive trend between incentive size and viral suppression (P-trend=0.0032), although the incentive groups did not significantly differ from each other. Small financial incentives delivered using mHealth can improve retention in care and viral suppression among adults starting HIV treatment. While further research should investigate the durability of effects from short-term incentives, these findings strengthen the evidence for implementing financial incentives within standard HIV care. From the implementation science evaluation, we found that biometric identification and mobile payments were acceptable to most patients and staff in this semi-rural region of Tanzania. Biometric identification and mobile payments may provide a scalable mechanism to improve patient tracking and efficiently implement cash incentives in low-income country settings, and mobile money payments may result in the unintended benefit of increasing savings and providing a means to control spending.
Retention in care and HIV viral suppression (<1000 copies per mL) at 6 months
Data are predictive marginal probabilities and 95% CIs estimated from logistic regression models adjusted for clinic. *N=464 participants retained in care at 6 months (86% of 530 total participants). †Primary outcome was the composite proportion of participants who remained in care at 6 months and had a viral load less than 1000 copies per mL.
Implementation Guidelines
Based on our mixed-methods implementation science results, recommendations for further implementation include: a) upfront effort needs to be expended to ensure that patient concerns about privacy are addressed, for example by allowing participants to opt-out of SMS notifications, or by providing assurance that SMS messages do not reveal anything about HIV status; b) while most participants had access to mobile phones and mobile money, providing access for all will be needed to successfully implement this system and consideration given to how to weigh this need against the ability to bring the intervention to scale; c) implementation support in the clinic including universal training, incentive payments for staff to use the system, and ensuring there is a solid understanding of the benefits conferred to patients (e.g., decreasing loss to follow up) will be crucial; d) getting the fingerprint system right took more time and was more complicated than expected – issues relating to image quality, computing storage and creating the threshold precision level for fingerprint recognition resulted in a steep learning curve; e) unexpected benefits of the system included lending a sense of legitimacy and belonging for patients, a strong understanding among clinical staff of how such a system could help patients and simplify clinic operations, and as a result of the mobile money, the potential for increased savings and increased control over spending, as well as increasing intra-household bargaining power for women.
Lessons Learned
Small, short-term financial incentives delivered using an mHealth system can improve 6-month retention in care and viral suppression among adults starting HIV treatment.
Although further research should investigate the durability of effects from short-term incentives, these findings strengthen the evidence for implementing financial incentives within standard HIV care.
The mHealth system including biometric identification and mobile payments was acceptable to staff and patients and increased the likelihood for scale. At the same time, these systems require special considerations regarding training of clinical staff, privacy for patients, and universal patient access to mobile phones.
Implications for Future Work
While further research should evaluate the durability of effects from short-term incentives, this study shows potential for a scalable financial incentive program to increase the use of HIV services and achieve viral suppression, a critical goal for ending the HIV epidemic.